 In the 21st century, healthcare professionals are witnessing a growing trend of musculoskeletal disorders (MSDs) that no longer respond effectively to traditional treatment methods. This phenomenon, which I term "treatment mismatch," arises from the rapid and profound changes in our environment and lifestyle. Understanding this concept is crucial for developing more effective therapeutic strategies that address the modern aetiology of these disorders. The Evolutionary Mismatch To comprehend the treatment mismatch, we must first explore the concept of evolutionary mismatch. For 99% of our evolutionary history, humans lived as hunter-gatherers in small, nomadic groups. This lifestyle, deeply intertwined with nature, shaped our physiology and behaviour. Our bodies evolved to respond to acute, short-term stressors with the fight-or-flight response, a mechanism designed to handle immediate physical threats. However, the last 10,000 years have seen a dramatic shift. We transitioned from a nomadic lifestyle to agrarian societies, then to industrialised cities, and now to an information age characterised by rapid technological advancement. These changes have occurred so quickly that our physiological adaptations have not had time to keep pace. As a result, our stress response, once advantageous for survival, has become maladaptive in the face of chronic, psychosocial stressors such as work overload, social pressures, and the constant connectivity of modern life. The Rise of Psychosocial Stressors In today's world, many MSDs are not caused by physical trauma but by psychosocial stress. Chronic stress, job insecurity, fear of change, and even frustrations like an internet outage trigger the same physical stress response our ancestors used to deal with immediate threats. This includes neurohormonal changes that tense muscles, alter vascularisation, and redistribute nutrients—all of which are inappropriate for addressing the subtler, chronic challenges of the modern environment. Traditional Treatments and Their Limitations Traditional treatment methods for MSDs, developed in the 19th and 20th centuries, were primarily designed to address biomechanical issues resulting from physical trauma. These methods include manual therapies, physical exercises, and ergonomic adjustments that focus on correcting mechanical dysfunctions and alleviating pain through physical means. While these treatments can be effective for conditions with a clear biomechanical origin, they often fall short in addressing MSDs driven by chronic stress and psychosocial factors. This is the crux of the treatment mismatch: therapies that worked well for the health problems of the past are less effective for the stress-related disorders prevalent today. Addressing the Treatment Mismatch To bridge this gap, manual therapists and healthcare professionals must adopt a more integral approach that integrates the understanding of psychosocial stressors and their impact on physical health. Here are several strategies to consider:
Conclusion The concept of treatment mismatch highlights the need for a paradigm shift in how we approach musculoskeletal disorders. By recognising the role of psychosocial stressors and adopting holistic, interdisciplinary strategies, we can develop more effective treatments that are attuned to the realities of modern life. Addressing this mismatch is essential for improving patient outcomes and promoting long-term health and wellbeing in the 21st century. References
By understanding and addressing the treatment mismatch, we can better serve our patients and adapt to the changing landscape of musculoskeletal health.
0 Comments
 Recently I've been reflecting on Dr. Robert Sapolsky’s views on free will. A subject he as described in his book "Determined: A Science of Life without Free Will" where he argues that free will is an illusion, positing that our choices and behaviours are entirely determined by biological and environmental factors beyond our control. I can follow his reasoning but then I got to wonder about how where the placebo effect would fit in his theory. This can seem paradoxical at first glance, but seems they can be reconciled. It was my believe that the placebo effect typically involved some level of expectation or belief influencing physiological outcomes, which might initially seem to require an act of free will. But if free will is an illusion, as Dr Sapolsky argues, then understanding how a placebo effect can still occur under determinism becomes an interesting puzzle... well I thought so anyway 😅 Understanding the Paradox Mind as a Product of the Body:
Placebo Effect:
Reconciling the Two Concepts Belief and Expectation as Biological Phenomena:
Supporting Sources
This article was written with the assistance of ChatGPT, but it represents my ideas, ensuring a blend of my scientifically informed insights and advanced AI support to bring it all together. 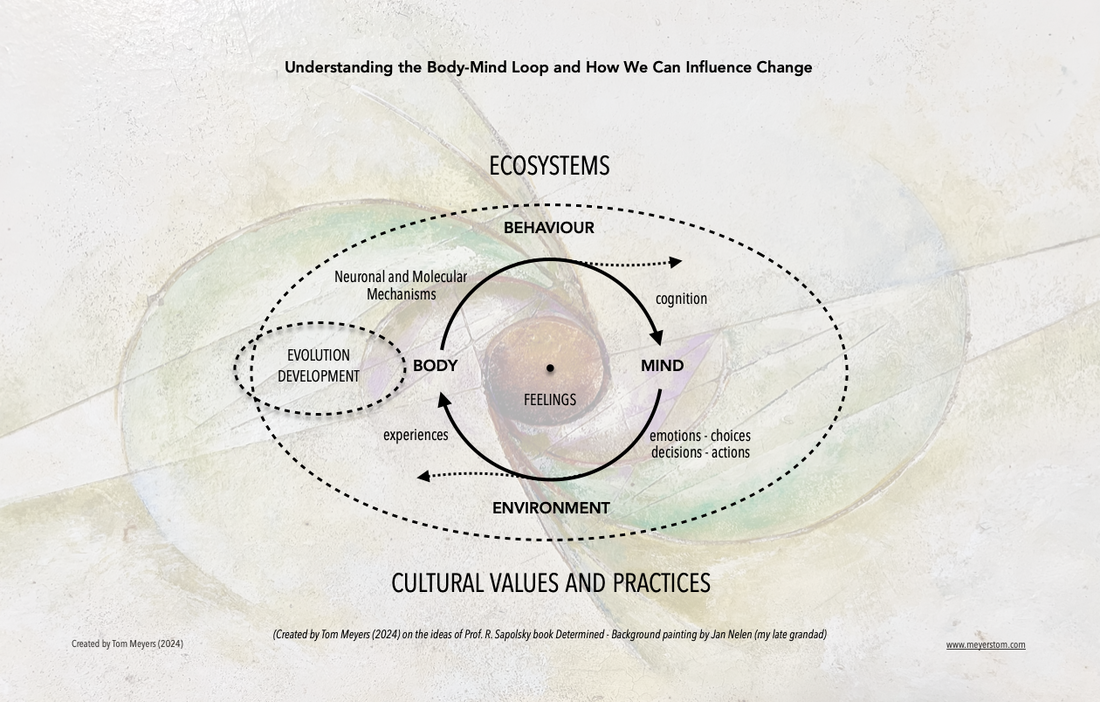 This is a work in progress based on my own thoughts and those of Professor R. Sapolsky’s books, including his latest, “Determined”, as well as A. Damasio’s “The Strange Order of Things” and elements of evolutionary and developmental mismatch theories. The purpose of this simplified diagram is to gain a better understanding of whether and how we can evolve on purpose to better adapt and manage change. It illustrates the continuous body-mind loop where our body’s neuronal and molecular mechanisms, influenced by genetics, environmental factors, and individual experiences, govern our behaviour. Behavioural changes affect cognition, which in turn shapes the mind. The mind’s decisions, choices, and actions then alter the environment, creating new experiences that continue to influence our body’s mechanisms. Throughout this process, feelings are generated and play a crucial role at each stage. At the moment, our rising “biological footprint” — a term I coined to capture the impact of our lifestyle, environment, and actions on our biological systems — is making us sick. By understanding the interconnected elements of my illustration, I hope you/we can better comprehend what is happening and why, but also gain insights into how you/we can purposefully change or stimulate a process of evolving on purpose (evolopsis). How do you feel about this? For example, by reading this, your body has created neuronal and molecular changes that alter your behaviour, perspective, emotions, choices, decisions, and actions, which in turn cause changes in your environment, creating experiences that further influence your body, changing the way you respond, and so on. What I’m striving for with this illustration is to shed light on my understanding of how you/we can foster better ways of adapting and managing change. In other words, how we can create stability through change and evolve with the changing times, thereby improving our physical and mental health and wellbeing and foster a more compassionate and humane society. Again it is a work in process… and I’m awaiting Prof. Sapolsky’s view on this. PS: The key message of Robert Sapolsky’s book Determined: A Science of Life Without Free Will is that human behaviour and decision-making are entirely shaped by a complex interplay of genetics, environmental influences, and individual experiences. Sapolsky argues that the concept of free will is an illusion, and our actions result from deterministic processes involving the body’s neuronal and molecular mechanisms, which influence behaviour and cognition.
 In our fast-changing world, stress has become a ubiquitous aspect of daily life. But why has stress, a general adaptive response meant to protect us, turned into a stressor that seems to harm us more than it helps? Does the answer lie in a conflict between biology and culture, or in other words, the concepts described in evolutionary medicine as evolutionary and developmental mismatches? Let’s take a look at these mismatch theories and see if they can shed light on the bigger picture. Evolutionary Mismatch: A Legacy of Our Past Evolutionary mismatch refers to the idea that the environment in which humans evolved differs vastly from the one we live in today. Our ancestors adapted to a world where immediate physical threats, food scarcity, and survival in the wild were the norm. The general adaptation response, involving the autonomic nervous system (ANS) and the hypothalamus-pituitary-adrenal (HPA) axis—more commonly known as the stress response and characterised by the "fight or flight" mechanism—evolved to handle these acute, short-term threats effectively. In the modern world, however, we face predominantly psychosocial stressors such as work pressure, financial concerns, and rapidly changing technological advancements that affect every aspect of our lives. These stressors are not typically life-threatening but are persistent, leading to prolonged activation of the general adaptation response. Our bodies, still wired for ancient dangers, respond to these modern stressors with the same neurohormonal and physical responses as they would to a predator attack, as there hasn’t been enough time for an evolutionary more apt adaptation to occur. This conflict between biology and culture, known as an evolutionary mismatch, may be one of the reasons for the rise in physical health problems today, including obesity, diabetes, and cardiovascular disease, as well as mental health problems such as chronic stress, anxiety, and depression. Developmental Mismatch: The Impact of Modern Lifestyles Developmental mismatch, on the other hand, refers to the discrepancies that occur during an individual’s growth and development due to the environment they are exposed to at various stages. A mismatch because experiences for which we create protective or defence mechanisms during critical periods of development are different than the conditions/ experiences encountered later in life. These developmental mismatches can disrupt normal physiological and psychological development, leading to long-term health issues, including obesity, metabolic disorders, cognitive impairment and behavioural disorders The Interplay of Evolutionary and Developmental Mismatches Does the interplay between evolutionary and developmental mismatches compound the problem of stress in modern society? Our evolutionary heritage predisposes us to respond to stress in ways that are no longer appropriate for most contemporary challenges. At the same time, developmental mismatches exacerbate our vulnerability to stress by disrupting healthy growth and development. This interplay may indeed explain the rise in stress-related physical and mental health problems and why traditional treatment solutions often fall short, as they fail to address the underlying evolutionary and developmental causes. To be continued... References:
This article represents the ideas researched by Tom Meyers and created with the assistance of ChatGPT, ensuring a blend of expert insights and advanced AI support. Tom Meyers is an osteopath (D.O. OSD, MSc. Ost), body-centred stress coach, and founder and instructor of The Reaset Approach, a therapeutic methodology and treatment modality designed to help individuals adapt, flourish, and thrive in the 21st century. Through workshops and writings, Tom aims to inform and revolutionise the field of manual therapy and empower therapists with the tools and knowledge to better serve their patients.
 Dive into the captivating journey of “Our Multigenerational Brain,” where the intricate workings of our minds mirror the rich dynamics of a family living under one roof. This enthralling exploration not only sheds light on the evolutionary marvel that is our brain but also draws a vivid analogy between its ancient and modern components and the generational interactions within a household. From the instinctual vigilance of the reptilian brain to the innovative spark of the neocortex, discover how these diverse elements of our consciousness clash, collaborate, and ultimately converge to guide us through the challenges of change. As we navigate the complexities of adapting to an ever-evolving world, this narrative offers a refreshing perspective on leveraging our inherent capacities for growth, resilience, and purposeful evolution. Uncover the art of balancing the wisdom of age with the curiosity of youth, not just to survive but to thrive in the face of the new and the unknown. “Our Multigenerational Brain” is more than an article; it’s an invitation to ponder, dream, and actively shape the future, embracing change not as an obstacle but as the essence of our humanity.
In the vibrant tapestry of human existence, the brain stands as a testament to our evolutionary journey, mirroring the complexities and dynamics of a multigenerational household. This fascinating analogy invites us to explore how different generations within a family — and correspondingly, different parts of our brain — interact, adapt, and evolve in the face of change. At the core of our beings, nestled deep within the brain, resides what could be linked to the wise and steadfast grandparent: the reptilian brain. This ancient part of our brain is tasked with our most primal functions — those that ensure survival. It‘s the instinctual guardian of our basic life processes, responding to the world with a simplicity that has ensured the continuation of our species for millennia. As we move through the layers of neural complexity, we encounter the limbic system, akin to the parental generation. This part of the brain enriches our lives with emotions and memories, guiding us through the social complexities of human relationships. It‘s the emotional heart of the household, fostering connections and ensuring the continuation of our deepest values and traditions. Then, at the pinnacle of this cerebral hierarchy, shines the neocortex: the vibrant, curious child, brimming with potential and a thirst for innovation. This is the seat of our creativity, our problem-solving abilities, and our capacity for complex thought. It‘s what enables us to look beyond the horizon, to imagine, plan, and dream. However, just as in any family, conflicts can arise. The reptilian brain, with its instinctual caution, often resists change, preferring the safety of the known. The neocortex, meanwhile, thrives on novelty and exploration, constantly seeking to expand the boundaries of our understanding and experience. This internal tension mirrors the generational dynamics within a household, where the wisdom of age and the boldness of youth must find a common ground. Just as the younger generation can introduce their elders to the wonders of new technology, showing them the benefits of adapting to change, the neocortex can guide the more primitive parts of our brain towards a more harmonious response to new challenges. But how can this be achieved without resorting to integrating technology? The answer lies in the art of gentle persuasion and the power of example. Just as a grandchild might patiently show a grandparent how to use a smartphone, highlighting its benefits and easing their fears, the neocortex can influence our more instinctual responses through gradual exposure to new experiences, scenarios, and future thinking — in other words, planning ahead — coupled with positive reinforcement. Imagine confronting a fear of heights not by shying away from high places, but by gradually and safely exposing oneself to them, thereby teaching the reptilian brain that these situations are not a threat. Or consider the enriching process of learning a new skill later in life, which, though it challenges the brain‘s established patterns, ultimately leads to growth and a profound sense of achievement. Similarly, envision crafting a “DNA for the future“ — the core elements of our being that remain constant, yet can be expressed in myriad ways. This approach offers a method to construct ‘if this, then that‘ scenarios, providing the stability and security the reptilian brain seeks when confronted with new challenges. In essence, the neocortex, with its capacity for reflection, planning, and foresight, can lead the way in adapting to change, teaching the rest of the brain that new experiences are not only manageable but also safe. This internal dialogue between the old and the new, the instinctual and the thoughtful, guiding our behaviour and actions going forward, can initiate a new step in our evolution. A step to flourish and thrive while the world around us is changing further and faster. Since our natural evolution is too slow, requiring generations to make the adaptive changes — time we do not have — the only option left to us is to help it evolve on purpose. It is what we are made to do. In weaving together the threads of our discussion, we arrive at a poignant reflection on the essence of human resilience and adaptability, as mirrored in the intricate dance of generations within both our families and our minds. As the neocortex, our beacon of innovation and foresight, harmonises with the ancient, instinctual parts of our brain, we‘re reminded of the perpetual interplay between tradition and transformation. This delicate balance propels us forward, urging us not merely to adapt to the changing landscapes around us but to thrive within them. Our journey through the multigenerational brain illuminates a profound truth: that embracing change is not just an act of survival but a testament to our inherent capacity for growth and evolution. It invites us to ponder, to dream, and to question how we can actively shape our future, rather than merely responding to it. In this moment of reflection, we‘re called to consider how our own internal dialogues, between the cautious wisdom of experience and the boundless curiosity of youth, can guide us toward a more harmonious and fulfilling existence. As the world whirls around us, faster and more unpredictably than ever, our challenge — and indeed, our opportunity — is to harness the collective wisdom of all parts of our brain. By doing so, we not only honour the legacy of those who came before us but also lay the groundwork for generations yet to come. In this light, our multigenerational brain doesn‘t just offer a metaphor for adaptation; it embodies a blueprint for flourishing and thriving in an ever-evolving world. So let us step forward, with courage and purpose, into the future we wish to create, embracing the change not as a force to be feared, but as the very essence of what it means to be human. I’d love to hear your thoughts on the analogy of the multigenerational family, as well as the emerging concept of ‘evolopsis’ that I am developing. Indeed, without the assistance of ChatGPT, this article might have remained just an idea in my brain. Shifting Perspectives: From General Adaptation Syndrome (GAS) to General Adaptation Process (GAP)4/4/2024  Fast-changing times necessitate new concepts to navigate the evolving health and wellbeing challenges they bring.In an era marked by rapid changes and unprecedented challenges, where technology is ever more present, our approach to health and wellbeing to flourish and thrive, necessitates rethinking. This includes the rethinking of our foundational models. Do these models still serve us, or do they need revision? For example, the traditional concept of the General Adaptation Syndrome (GAS), introduced by Hans Selye, has long served as a foundational model in understanding stress and its effects on the human body. GAS outlines a three-stage reaction to stress: alarm, resistance, and exhaustion. While these stages haven’t changed, I believe as we navigate the complexities of modern life, wouldn’t a more positive, dynamic and proactive term or designation be more constructive? This article reflects on the benefits of transitioning from GAS to the General Adaptation Process (GAP) as a more fitting model when talking about stress. Understanding the Limitations of GAS With GAS stress is presented as a linear, somewhat predictable process with a clear endpoint. While this model has significantly advanced our understanding of stress-related illnesses and the body's response mechanisms, I feel it falls short in encapsulating the fluidity and variability of human experiences with stress in the 21st century. The designation of "syndrome" provokes in me that it is a pathological condition, potentially overshadowing the adaptive and positive aspects of dealing with stressors. Stress is after all essential to adapt and manage change and is not per se the problem. That the stress response hasn’t evolved at the same speed as the challenges we created, and the physical reaction it engendered due to our increasing biological footprint (see my previous article) and that it is triggered for things it doesn’t need to, that is the true issue we need to focus on. Introducing the General Adaptation Process (GAP) Instead of GAS, I propose another way of saying the same thing but with a more positive and constructive connotation, f the General Adaptation Process (GAP). Using the process instead of syndrome means the stress response is seen not as a finite sequence of stages but as an ongoing, cyclical process of learning, growth, and resilience-building. This shift in terminology from "syndrome" to "process" can also reflect a more nuanced understanding of how individuals interact with, adapt to, and recover from stressors over time. GAP embraces the complexity of these interactions, recognising them as integral to personal development and wellbeing. Embracing Complexity and Individuality As each individual’s encounter with stress is unique, influenced by a myriad of genetic, environmental, and personal factors, it is maybe also a good idea to move away from the more static model GAS represents. I feel that GAP allows for a more personalised understanding of stress, emphasising the importance of individual pathways to resilience and adaptation. Highlighting the Dynamic Nature of Adaptation By viewing adaptation as a process, GAP accentuates the dynamic and ever-changing nature of how we respond to life’s challenges. It encourages proactive engagement with stressors, highlighting the capacity for learning and growth inherent in each stress encounter. This perspective fosters a more optimistic outlook on stress, seeing it as an opportunity for personal development rather than solely a risk factor for disease. Encouraging an Integral Approach For me, GAP promotes a more integral approach to stress management, integrating physical, psychological, and social strategies. This encompasses a broad range of practices, from physical activity and nutrition, social support to creating a DNA for your future to futurize yourself, underscoring the multifaceted nature of effective adaptation. I also believe that GAP offers a more positive approach for individuals to conquer setbacks and will help them in the process of emerging from challenging situations with increased strength, skills, and wellbeing. By focusing on the process of adaptation, GAP emphasises the potential for positive transformation through the experience of stress. Conclusion
As we face new and complex challenges in health and wellbeing, adopting the General Adaptation Process as term or designation offers a more empowering and comprehensive framework for understanding and managing stress. Shifting from seeing stress as a syndrome to a process not only reflects a deeper understanding of the nuances of human adaptation but also aligns with a proactive and optimistic approach to life’s challenges. This shift encourages individuals to embrace the journey of adaptation as an opportunity for growth, resilience-building, and ultimately, a more fulfilling life. In doing so, we acknowledge that the path to wellness is not merely about surviving stress but thriving through it, harnessing our experiences to foster a richer, more adaptive existence.  The concept of the “Biological Footprint,” which I introduced to capture the impact of our lifestyle, environment, and actions on our biological systems, delineates the influence of human activities and lifestyle choices on our inherent natural resources that are vital for health. This concept draws a parallel with the well-established notion of the “ecological footprint,” but it specifically focuses on our biological wellbeing as opposed to earth. This innovative idea sheds light on how the demands of our lifestyle, work, and ecological challenges caused by the anthropogenic environmental changes exert pressure on our innate resources, crucial for maintaining health and wellbeing. At present, our biological footprint is expanding, thereby straining our innate resources and leading to a.o. increased levels of stress, anxiety, musculoskeletal disorders, mental health problems and diminished wellbeing. With this concept I hope to introduction a deeper examination of how our everyday choices impact not only the environment but also our personal health in significant ways. It serves as a rallying cry for the adoption of more sustainable and health-conscious practices that benefit both our planet and ourselves. Creation and Purpose Through the development of The Reaset Approach, unveiled the idea of the Biological Footprint as a means to encapsulate the effects of our modern, often stress-laden lifestyles on our natural coping and adaptation resources, including the general adaptation syndrome (fight-flight response). The Reaset Approach itself heralds a paradigm shift in manual therapy, aiming to reaset the autonomic nervous system (ANS) and tackle the root causes of physical and mental health issues stemming from our contemporary way of living. The Biological Footprint concept was crafted to illuminate how our environment – encompassing work, technology, diet, physical inactivity, family life, lifestyle, and exposure to anthropogenic environmental changes – accumulate and manifest as tangible impacts on our health and wellbeing. Importance of Understanding the Biological Footprint Grasping the significance of one‘s Biological Footprint is crucial for multiple reasons:
Comparison with Ecological Footprint While the ecological footprint quantifies the environmental impact of human activities in terms of the land area needed to sustain their natural resource use, the Biological Footprint concentrates on the “internal environment.“ It evaluates the cumulative impact of lifestyle choices on an individual‘s biological systems, particularly the autonomic nervous system, crucial for stress response and overall health. Both concepts are underpinned by the principle of sustainability—just as we strive for a planet-sustainable lifestyle, we should also aspire for a body-sustainable lifestyle. Reducing Your Biological Footprint: A Pathway to Holistic Health Reducing your Biological Footprint transcends immediate work-related, lifestyle, and environmental changes, delving into a deeper transformation of your approach to life and wellbeing. The methodologies of developing a “DNA for Your Future“ and “Futurizing Yourself“ could play an important pivotal role in this journey, offering a forward-looking strategy for sustainable health and wellness. Developing a DNA for Your Future Creating a “DNA for Your Future“ involves thinking about what you want to feel, your aspirations and potential that do not alter but can be expressed in different ways over time. This strategy is the basis for Futurizing Yourself and through it you can:
Futurizing Yourself “Futurizing Yourself“ entails crafting a vision for your future based on your DNA for the future. By adopting this mindset, you can:
Practical Steps to Reduce Your Biological Footprint Merging the strategies of "Futurizing Yourself" and developing a "DNA for Your Future“ with existing actionable health-oriented measures can substantially reduce your Biological Footprint:
Conclusion Embracing the concept of reducing your Biological Footprint revolutionises your approach to health, turning the lens from a planetary scale to a deeply personal one. Unlike Planetary Health, which aims to understand and mitigate human activity‘s effects on Earth‘s natural systems, reducing your Biological Footprint spotlights your individual actions and their direct impact on your personal health and wellbeing. This nuanced view prompts us not just to consider how our lifestyles impact the planet but also to contemplate their resonance within our biological ecosystems. It beckons us to recognise that there is a relationship between our planetary sustainability and the stewardship of our own health. Aligning your daily choices with the tenets of both personal and planetary wellbeing not only contributes to the broader mission of Planetary Health but also sets us on a transformative path towards a more balanced and sustainable existence for ourselves. In this light, reducing our Biological Footprint emerges as a crucial component of the global endeavour to heal our planet, reminding us that our steps towards personal health optimisation have far-reaching effects, enhancing the collective wellbeing of our global community and the Earth itself.  Note: This article was made in collaboration with ChatGPT.
 Background The concept of peripersonal space, an area of space immediately surrounding us, is not just a physical boundary but a dynamic interface through which we interact with our environment. This space is neurologically represented and actively mapped by the brain, allowing us to navigate our surroundings, perform tasks, and communicate with others effectively. The understanding of peripersonal space has profound implications for manual therapy, particularly in innovative approaches like The Reaset Approach, developed by Tom Meyers. Introduction In manual therapy, the traditional focus has been on addressing physical ailments through direct manipulation of the body's structures. However, The Reaset Approach introduces a paradigm shift, emphasising not just the physical but also the neurological and psychological aspects of healing. The concept of peripersonal space becomes relevant here as it extends the domain of therapy beyond the tangible, into the realm of the patient's sensory and spatial perception. Content The Neuroscience of Peripersonal Space: Research in neuroscience reveals that peripersonal space is monitored by a network of brain areas that process information about objects close to the body. This network is involved in integrating sensory inputs with motor actions, highlighting its significance in manual therapy, where touch and movement are central elements. Peripersonal Space in The Reaset Approach: The Reaset Approach, with its holistic perspective on healing, recognises the importance of peripersonal space in therapy. By recognizing and respecting this space The Reaset Approach practitioner creates a feeling of safety and trust which is crucial when the objective is lifting the autonomic lesion and creating autonomic balance. By acknowledging this space and effectively tuning into it a practitioner facilitates the necessary conditions for a deeper level of healing that transcends physical manipulation. Implications for Manual Therapy: Understanding and respecting the patient's peripersonal space can lead to improved therapeutic outcomes. It allows therapists to be more attuned to the subtle cues that patients emit, enabling a more nuanced and effective treatment strategy. Moreover, this awareness can enhance the patient's sense of safety and comfort, crucial elements in the healing process. Conclusion The Reaset Approach is comprehensive therapeutic methodology, developed in response to the evolving nature of patients' health challenges, and a hands-on treatment modality with a focus on reasetting autonomic balance before addressing their symptoms. By its integration of the neurological and psychological aspects of peripersonal space into treatment The Reaset Approach stands truly takes manual therapy into the 21st century. As manual therapists, the challenge and opportunity lie in exploring how this understanding of peripersonal space can be incorporated into daily practice. How would you use this information into your practice today? This question invites reflection and experimentation, encouraging therapists to broaden their therapeutic horizons and enhance the well-being of their patients through a deeper understanding of the human body and mind. More information:
di Pellegrino, G., & Làdavas, E. (2015). Peripersonal space in the brain. Neuropsychologia, 66, 126–133. https://doi.org/10.1016/j.neuropsychologia.2014.11.011 Rabellino, D., Frewen, P. A., McKinnon, M. C., & Lanius, R. A. (2020). Peripersonal Space and Bodily Self-Consciousness: Implications for Psychological Trauma-Related Disorders. Frontiers in neuroscience, 14, 586605. https://doi.org/10.3389/fnins.2020.586605  In today’s fast-changing world, the nature of health challenges has shifted significantly from the 20th-century paradigm. Previously, health issues predominantly stemmed from external physical forces, leading to somatic dysfunction. However, in the 21st century, a crucial transformation has occurred. The prevailing dis-ease patterns are now rooted in internal stress-related alterations, specifically autonomic dysfunction, marking a fundamental distinction. Traditional treatment approaches, designed to address functional and structural changes resulting from somatic dysfunction triggered by external factors, fall short in tackling the intricate multimodal health issues stemming from autonomic dysfunction associated with adaptive and psychosocial stress. In other words, a “treatment” revolution is needed to address the shift from external to internal dis-ease patterns. Within this shifting landscape, The Reaset Approach emerges as a therapeutic methodology and treatment modality in response to the changing needs, directing its focus to the autonomic lesion – an internal alteration that lies at the core of contemporary physical and mental health challenges, without losing sight of the fact that a patient may still present with a predominantly somatic dysfunction. In the realm of manual therapy, the usual treatment approach puts emphasis on altered structural or functional patterns triggered by external forces. Manual therapists’ treatment of these altered physical patterns is mainly based on a form of manipulation to restore balance. The Reaset Approach brings about a paradigm shift in response to the constantly evolving nature of today’s health challenges. Instead of solely attributing issues to external forces, the author has introduced the term “autonomic lesion” to emphasise the role of the autonomic nervous system (ANS) in the changing health landscape. The autonomic lesion, evolving into an autonomic dysfunction, has emerged as the primary contributor to contemporary, often multimodal health problems. These issues extend beyond mere physical health and wellbeing, impacting behaviour, cognition, emotions, time perception, and social interaction. The deliberate focus on the autonomic balance in The Reaset Approach, and thus on resolving the autonomic lesion and consequent autonomic dysfunction, is gaining significance in today’s fast-changing and challenging world. The author points out that the stress response has itself become a stressor because of a conflict between our slow-evolving biological evolution and the exponential speed at which our culture (environment) is changing. The rapid pace of modern life has surpassed our biological capacity to adapt. The conflict that arises translates itself into the “autonomic lesion” and develops into a specific kind of autonomic dysfunction: stress-related dysautonomia (S-RD). It is this stress-related dysautonomia that has become the main direct and indirect cause of a wide range of physical and mental health problems (psychosomatic dysfunctions) in the 21st century, in contrast to the external physical forces leading to somatic dysfunction of the 20th century. The success of a treatment is interdependent on the treatment of the S-RD, i.e. the “reaset” (return to ease) of the autonomic dysfunction and lifting of the autonomic lesion. With a primary objective of “reasetting the ANS first and maintaining it during treatment”, The Reaset Approach addresses the paradigm shift that 21st-century healing methods need and initiates the revolution in the evolution of manual therapy for improved patient outcomes. In today’s fast-changing world, where adaptive and psychosocial stress has become central to dis-ease patterns, reasetting the ANS has become essential and key to helping patients cope with the challenges of modern life and thus preventing dis-ease from settling in. Where dis-ease has already set in, reasetting the ANS should be included in the treatment modality as a pre-treatment before addressing the patient’s symptoms. Rooted in the principles of pioneers like Dr A.T. Still and Dr R. Virchow, The Reaset Approach has emerged through a journey of continuous exploration over 16 years, after the author’s patients reported that his way of working was different from that of his colleagues and other more conventional manual therapy methods. This echo still resounds today in new patients who find their way to him and his students. The author, founder and practitioner of The Reaset Approach, Tom Meyers, is now presenting workshops internationally to share this therapeutic methodology and treatment modality, taking it beyond his own treatment room and out into the world. He also has committed himself to helping reshape educational curricula worldwide to include the importance of initiating autonomic balance in today’s changing aetiology of disease patterns. “Taking yourself and your skills into the 21st century” and “initiating a revolution in the evolution of manual therapy” are not merely slogans for the author but an ongoing message and narrative, inviting all to join in an exploration of the changes needed to meet today’s health and wellbeing challenges and those emerging in the future. Author: Tom Meyers Discover more about Tom and/or The Reaset Approach at www.thereasetapproach.com References: Hallman, D. M., & Lyskov, E. (2012). Autonomic regulation, physical activity and perceived stress in subjects with musculoskeletal pain: 24-hour ambulatory monitoring. International journal of psychophysiology : official journal of the International Organization of Psychophysiology, 86(3), 276–282. https://doi.org/10.1016/j.ijpsycho.2012.09.017 Liem, T. (2016). A.T. Still's Osteopathic Lesion Theory and Evidence-Based Models Supporting the Emerged Concept of Somatic Dysfunction. The Journal of the American Osteopathic Association, 116(10), 654–661. https://doi.org/10.7556/jaoa.2016.129 Liem, T., van den Heede, P., et al. (2017). Foundations of Morphodynamics in osteopathy. An integrative approach to cranium nervous system, and emotions. Handspring Publishing. Meyers, T. (2019). The effect of the “Reaset Approach” on the autonomic nervous system, neck-shoulder pain, state-trait anxiety and perceived stress in office workers: A randomised controlled trial. MSc. Thesis. Dresden International University (DIU) and Osteopathy Schüle Deutschland (OSD). https://bit.ly/47r8juO Waitzkin, H. (2006). One and a Half Centuries of Forgetting and Rediscovering: Virchow’s Lasting Contributions to Social Medicine. Classics in Social Medicine. https://www.medicinasocial.info/index.php/socialmedicine/article/view/6/7 Author Tom Meyers (born in 1970), as well as being a Belgian Osteopath D.O., MSc. Ost., and body-centred stress coach who runs a private practice in Brussels, is also a visionary on a mission to help people flourish in the flow of evolution and thrive in this fast-changing, uncertain and challenging world.   Introduction In today's fast-paced world, stress has become an omnipresent companion for many. From hectic work schedules to personal responsibilities, the pressures of modern life can take a toll on both our mental and physical well-being. For manual therapists (physiotherapists, osteopaths, fascia and craniosacral therapists…) understanding the intricate relationship between stress-related dysautonomia and its connection to evolving disease patterns is essential. This article delves into the significance of this interplay, particularly concerning patients with musculoskeletal pain, highlighting why mechanistic therapy modalities might fall short in such cases. Stress-Related Dysautonomia: Unravelling the Connection Stress, that omnipresent force, has a profound impact on our bodies, and at the heart of its effects lies the autonomic nervous system. Chronic stress, characterised by an imbalance in the autonomic nervous system, can result in stress-related dysautonomia (SRD). SRD is the condition where the sympathetic nervous system, responsible for the fight-or-flight response, is in a state of over-activation, while the parasympathetic nervous system, governing rest and relaxation, is permanently under-activated. This imbalance manifests in symptoms such as musculoskeletal pain to headaches or migraines, lack of energy, sleep disturbances, stomach or bowel problems, cardiovascular disease, mood swings, cognitive impairment, brain fog, depression, anxiety, etc. The Changing Landscape of Disease Patterns Disease patterns are not static; they evolve over time due to a complex interplay of factors including lifestyle changes, societal stressors, and environmental shifts. Stress, a potent contributor to many health issues, including dysautonomia, weakens the immune system and triggers inflammation. Chronic stress can thus contribute to the development or exacerbation of conditions ranging from cardiovascular diseases to autoimmune disorders and mental health problems. As these disease patterns change, manual therapists must be prepared to adapt their approaches to effectively address emerging health concerns. The Manual Therapist's Role in Stress-Related Musculoskeletal Pain The influence of stress-related dysautonomia is an emerging phenomenon that is increasingly prevalent as a primary contributor to a.o. musculoskeletal pain in patients. These individuals may exhibit pain that mirrors typical musculoskeletal discomfort, yet it defies conventional treatment approaches. The intricacies of this challenge arise from the intricate interplay between their musculoskeletal system and the autonomic nervous system's involved in the bodies stress response. Why Mechanistic Therapy Modalities Fall Short Traditional mechanistic therapy modalities, which primarily focus on the biomechanical aspects of pain, might not yield optimal results for patients with stress-related musculoskeletal pain. This disconnect arises because these modalities fail to address the underlying dysautonomia-driven component of the pain. Approaches that solely target the physical symptoms without considering the role of the autonomic nervous system are likely to provide only temporary relief and often fall short in the long term. The Holistic Approach: Bridging the Gap A revolution in the evolution of manual therapy is needed to address this emerging phenomenon. Manual therapist need to become well-versed in a more body-centred stress coaching approach. To stay relevant they need to take themselves and their skills to next level to offer the best care for their patients and their professional reputation. Recognising the influence of stress on the autonomic nervous system and subsequently on pain perception allows manual therapists to provide the evolving care this fast-changing world needs with a more integrative approach to well-being. In other words a manual therapists need to evolve with their time to empower patients to flourish and thrive and navigate the challenges of life by addressing both the symptom and its origin. Conclusion The shifting landscape of disease patterns underscores the critical need for a profound grasp of stress-related dysautonomia, especially within the realm of musculoskeletal pain. Manual therapists who demonstrate a heartfelt dedication to their patients and possess the necessary tools are positioned as key influencers in the trajectory of future health and wellness. By incorporating a targeted therapeutic approach capable of reasetting the autonomic nervous system into their practice, they hold the potential to catalyse flourishing and resilience in an ever-evolving world. Yet, the magnitude of their influence hinges intrinsically on their openness to embracing a forward-thinking approach to their practice, one that aligns with the currents of change and adaptation. In summary, the evolving dynamics of health and stress demand a holistic comprehension of stress-related dysautonomia, primarily concerning musculoskeletal pain. Manual therapists, armed with both genuine dedication and specialised tools, can emerge as beacons of better health and vitality in an ever-shifting landscape. The true measure of their impact lies in their willingness to pioneer a futurized approach within their practice. Are you a manual therapist ready to take yourself and your skills to the next level? Visit www.thereasetapproach.com and register for one of the upcoming workshops, or reach out to [email protected] for more information or to suggest a workshop location near you. Your journey towards a more impactful and fulfilling practice begins today. Disclaimer This article was written by and created on Tom’ Meyers’ insights and experiences based on information provided by ChatGPT. The information provided is intended for educational and informational purposes only. The views expressed in this article are those of the co-authors and do not constitute professional medical advice or diagnosis. Manual therapists and healthcare practitioners should exercise their clinical judgment and consult appropriate sources for personalised recommendations. The authors do not endorse any specific products or services mentioned in this article. For any health-related concerns, readers are advised to consult with qualified healthcare professionals. DOWNLOAD THE ARTICLE
|
Archives
July 2024
Categories |
||
 RSS Feed
RSS Feed
